
Not every condition responds predictably to standard care. Sometimes, your body won’t listen to your brain — or your brain won’t listen to your body. Maybe it’s an ache that doesn’t sleep or a twitch that interrupts a sentence. When that happens, it’s worth exploring other tools.
One of them is neurostimulation, a method that uses mild electrical or magnetic pulses to modulate the activity of certain nerves or brain circuits, aiming to improve their function. Neurostimulation might not be the first idea on the list, but relief doesn’t always arrive in obvious ways. As such, it might be one more tool that could change what daily life feels like quietly, gradually, and on your terms.
-
Neurostimulation targets the problem areas in your nervous system — a small device sends controlled pulses to help the body send and receive messages in a more organized way.
-
Not all neurostimulators have the same purpose, each is built for a different kind of problem. Knowing which one fits depends on where the issue starts and what needs adjusting.
-
If other treatments haven’t helped enough, neurostimulation might be worth considering. Consult your healthcare provider to determine if it can be a right fit for your condition.
What is neurostimulation, and how does it work?
It makes more sense to talk about neurostimulation once we’ve looked at the system it interacts with.
The nervous system is how your body remains in sync. It’s a web of connections between your brain, spinal cord, and nerves. Basically, the brain acts as a command hub that decides what needs to happen. The spinal cord receives and relays instructions from the brain down your spine, sort of acting like a main road. Then your nerves branch out from there, delivering instructions to your muscles and organs and sending back updates.
These messages run everything: movement, pain, temperature, bladder control, balance, speech, and even your heartbeat. Most of the time, you don’t notice any of it. You tap your foot. You feel the wind. You hold in a sneeze during a meeting. You withdraw your hand when touching something hot. All of that, without thinking.
But when the nervous system loses its rhythm, when the messages are too fast, too slow, or just plain wrong, it can show up in unexpected ways. Pain that lingers. Muscles that stiffen or tremble. Nerves that stop responding altogether. Sometimes, the problem starts in the brain. Other times, it’s further down the line. Either way, the result is the same: your system starts to send the wrong messages and becomes less efficient at filtering abnormal ones out.
Neurostimulation is a way to help manage these faulty signals.
Research shows that neurostimulation uses small, controlled electrical pulses to modulate nerve activity. A device (usually implanted under the skin or positioned near a specific nerve or brain area) sends electrical pulses to modulate abnormal neural activity. Instead of blocking nerves entirely, it fine-tunes their signals, calming signals that are too loud, encouraging ones that are too quiet, or helping the brain filter what it should pay attention to.
Expert insight
“Neurostimulation has reshaped how I view the spectrum of functional brain interventions,” says Louis Costello, MD, when asked about this topic. “For patients with refractory neurological conditions, particularly when pharmacologic tolerance or sensitivity creates bottlenecks, neuromodulation can offer a sustained circuit-based modulation without the systemic wear and tear of chronic drug exposure,” he adds.
When thinking about the upcoming decade, he expects “device-based treatment to move closer to front-line care, especially as parameters become more targeted. I would say the real shift lies in making brain signal calibration feel less experimental and more routine, like correcting posture, only inside the cortex.”
Getting acquainted with neurostimulators
All neurostimulator systems have three main components, and each plays a specific role in how the treatment works:
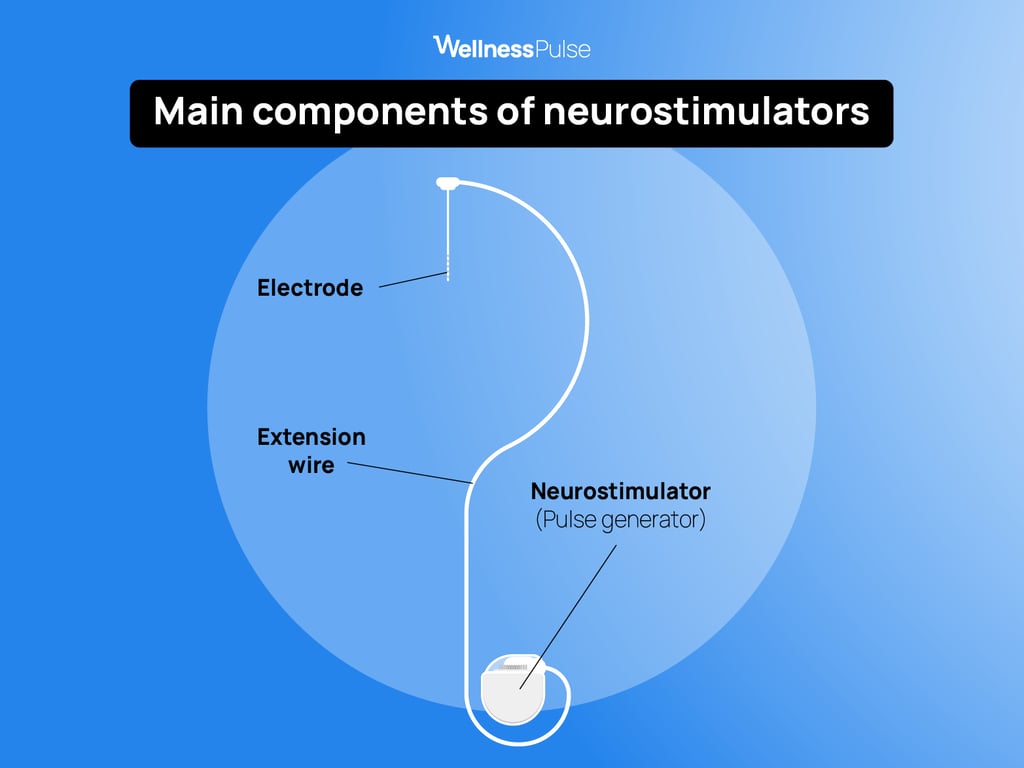
- The generator is the actual neurostimulator. This is simply the device that gets implanted under the skin, usually in areas like the chest or lower back. This is what produces the electrical signals that help modulate nerve activity.
- The leads are the thin wires that deliver those electrical signals to carefully selected areas of the nervous system. Their placement depends on the condition being treated and is precise enough to influence the target nerve activity.
- The programmer is the handheld controller. This lets the person using the system adjust the settings themselves, changing the intensity, turning it on or off, or switching between different programs.
Types of neurostimulation devices and their applications
Neurostimulation exists in different forms, as not every condition affects the same part of the nervous system. Some devices focus on the brain, others on the spinal cord or individual nerves. The goal is always the same: to adjust how signals are transmitted and received. Let's look at some of the widely used ones and their applications.
Spinal cord stimulation (SCS)
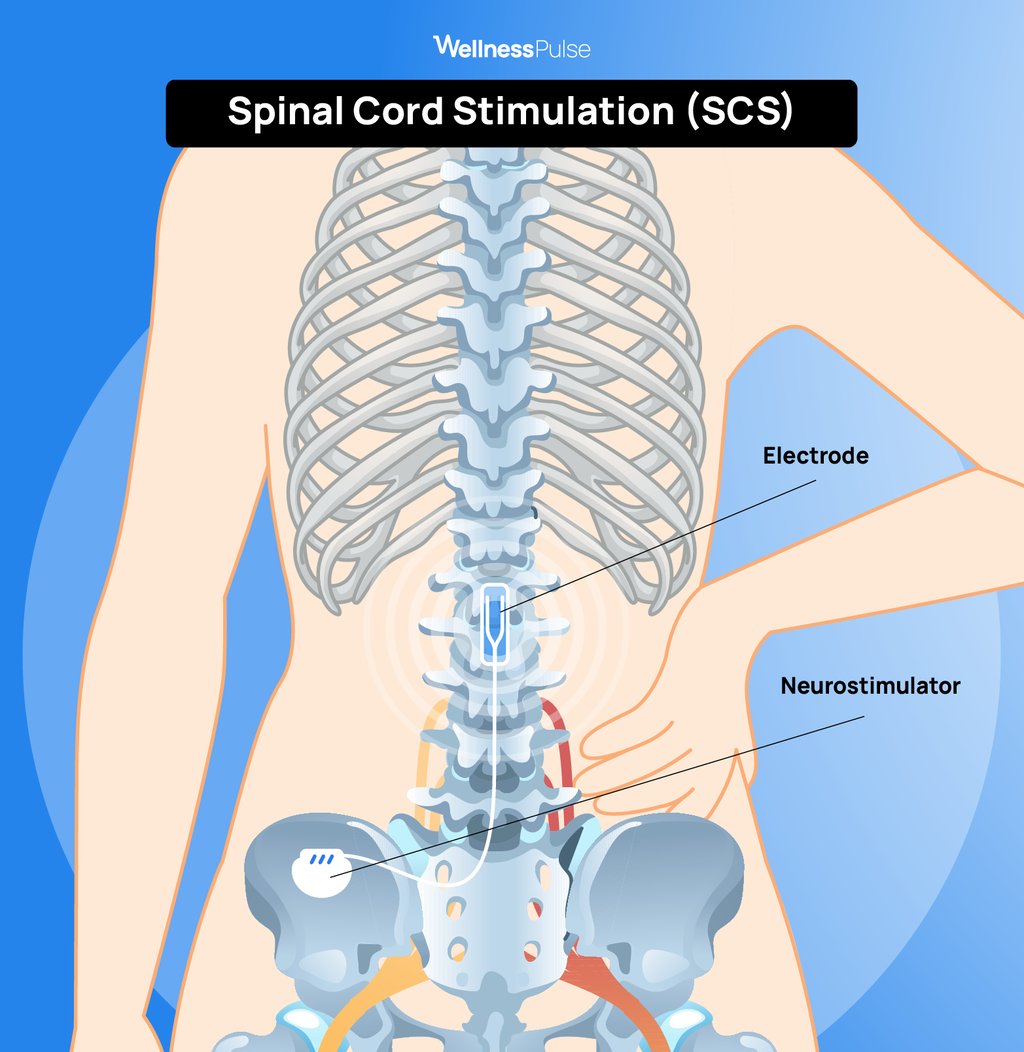
This is often used for nerve pain that remains long after surgery or when healing is already completed. A small device is implanted under the skin, with common areas being the lower back or just above the buttocks. This is then connected to thin insulated wires that sit close to the spinal cord in the epidural space.
How it works
The spinal cord acts as a major relay between the body and the brain. Pain signals pass through it on their way up. What spinal cord stimulators do is send mild electrical impulses to that area to interrupt those signals. The pain isn’t erased, but it’s changed, often felt as a softer tingling or buzzing instead of something sharp or constant.
Who it’s for
SCS is usually considered after other treatments for neuropathic chronic pain management haven’t helped enough. Studies have shown that this type of stimulation can be commonly used for:
- Back or leg pain that continues after spinal surgery (failed back surgery syndrome)
- Nerve pain from diabetes
- CRPS (complex regional pain syndrome)
- Post-surgical or injury-related nerve pain
- Some cases of vascular pain in the limbs
One study explored the efficacy of neurostimulation in chronic pain relief over three years. It involved 52 individuals who were followed up over the course of 36 months. Three outcomes were measured, including the pain rating scale, depression index, and disability index. The study found that there was a significant improvement across all the evaluated areas, rendering SCS an effective long-term treatment for spinal pain relief.
How the process works
There’s a short trial phase before anything permanent is implanted. A temporary version of the device is placed to see if it makes a noticeable difference. If the results are positive, a longer-term system can be implanted in a minor procedure. Individuals also receive a remote control to adjust the intensity themselves; some prefer more stimulation during certain activities, others less. It’s flexible.
Deep brain stimulation (DBS)
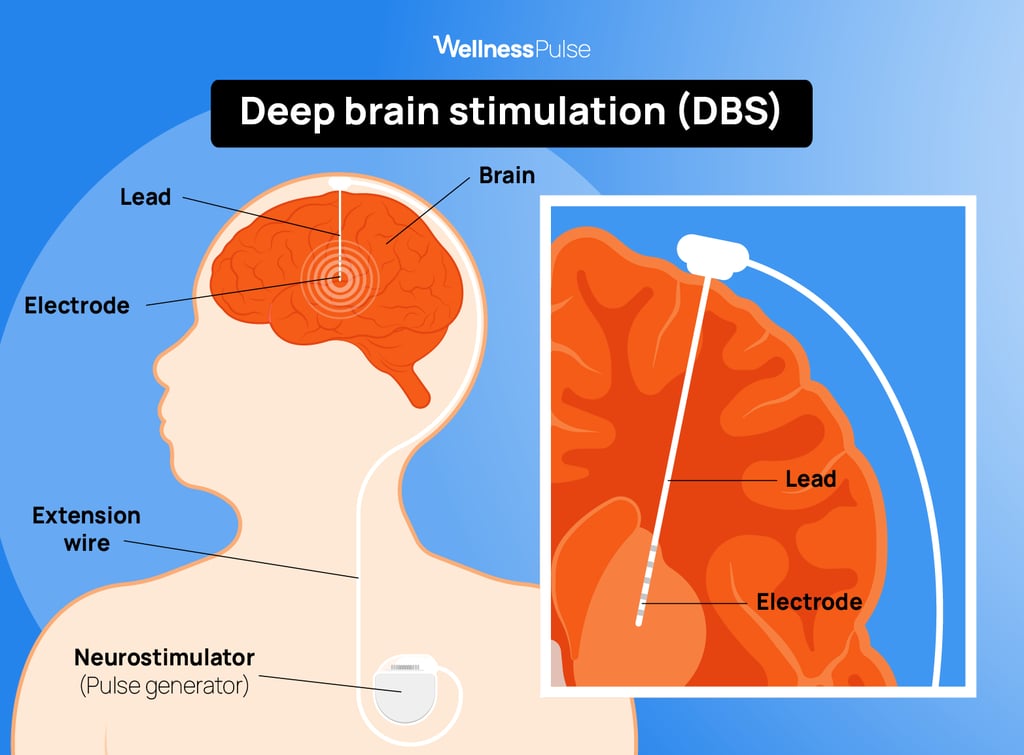
This approach is used when certain areas of the brain aren’t working together as well as they should, which is often witnessed in movement disorders such as Parkinson’s disease or essential tremor. It involves a surgical procedure where fine electrodes are placed in specific parts of the brain that help control movement. These are connected to a small device, usually implanted under the skin near the collarbone. The device sends regular electrical pulses that help bring those brain signals back into a more balanced rhythm.
How it works
In conditions like Parkinson’s disease, some brain circuits become overactive or irregular. The stimulation isn't about silencing the signals completely but rather stabilizing the rhythm. Over time, this can suppress bothersome symptoms such as tremors, stiffness, and uncontrollable movements.
During the procedure, electrodes are usually situated in the subthalamic nucleus or globus pallidus, which are regions of the brain partially responsible for movement. The purpose is not to shut anything off but to allow these signals to fire in a more synchronized pattern.
Who it’s for
DBS is usually considered after medications have been tried for a while and either aren’t working well or are causing problems of their own. Research reveals that it’s most often used for:
- Parkinson’s disease
- Essential tremor
- Dystonia
- Severe, treatment-resistant OCD
It’s not a first step, but for the right person, it can be a helpful next one. DBS has been increasingly resorted to in recent years for its hopeful promise to decrease the symptoms of Parkinson's and their impact on those living with the disease. More recent studies have revealed further potential in adaptive DBS for Parkinson's, which calls for a more personalized approach to DBS according to individual cases.
How the procedure works
Before anything is done, detailed brain imaging is used to figure out exactly where the electrodes should go. The first surgery places those leads in the brain. A second procedure implants the pulse generator under the skin and connects it to the leads.
The system is then programmed and adjusted over several appointments; the stimulation settings are individual and can be changed as symptoms change.
What it can offer
DBS doesn’t cure the condition, but it can give people more control over their symptoms. Some need less medication. Some move more freely. Some just feel like things have settled a bit, which can make a big difference in daily life.
The stimulation is adjustable and reversible. If things change down the line, the settings can be adapted, or the system turned off altogether. Nonetheless, not everyone is a candidate for DBS. The decision must be carefully made, considering individual medical, neurological, and psychological circumstances with the guidance of a medical team.
Vagus nerve stimulation (VNS)
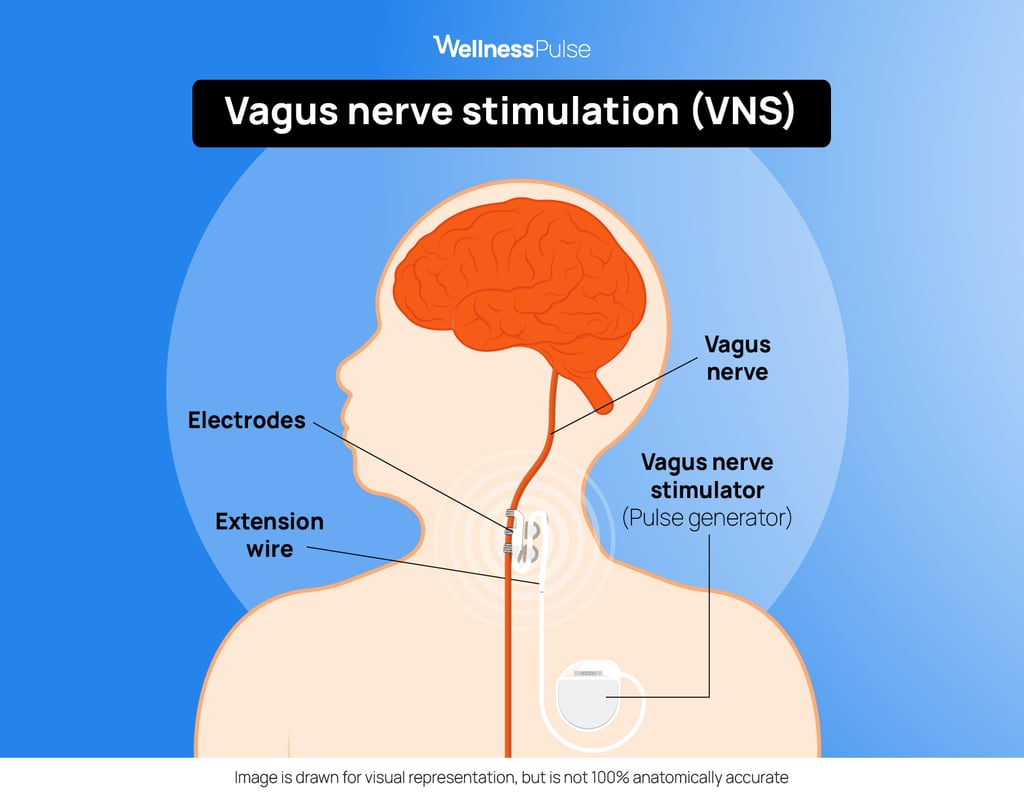
VNS is sometimes resorted to when treatment used in epilepsy or depression isn’t improving enough with medication alone. The device to be implanted is small, with a thin wire extending from it to the vagus nerve in the neck. This is one of the nerves that carry signals between the brain and several organs. The device then releases mild electrical pulses at regular intervals whenever it's turned on.
How it works
The vagus nerve helps regulate brain areas involved in mood, alertness, and mechanisms related to seizures. With stimulation, VNS will reduce seizure frequency in people with epilepsy, whereas for treatment-resistant depression, it may establish more stable brain activity in the long run.
The stimulation is done in the background and works to provide a series of brief pulses at regular intervals throughout the day. A tingling sensation, light voice, or throat flutter upon activation has been reported, but these are typically temporary and only minimally discernible.
Who it’s for
VNS is usually considered after other treatments have been tried. It’s most commonly used for:
- Drug-resistant epilepsy. A large prospective study of 362 individuals showed improved seizure control over three years, with responder rates increasing to about 58.8%, emphasizing the potential of VNS in helping manage these symptoms.
- Treatment-resistant depression, for which VNS is an FDA-approved treatment. Several studies have also advocated for the positive role of VNS as an adjunct therapy alongside antidepressants, where many have reported improved quality of life and reduced suicidal ideations.
The procedure
The device is fitted through a minor surgical procedure — one small incision in the chest and one in the neck. After recovery, it’s activated and adjusted gradually over several appointments to find the right settings. You’ll also have a handheld magnet or remote to control or pause the stimulation if needed, but once things are stable, most people don’t need to think about it day to day.
Peripheral nerve stimulation (PNS)
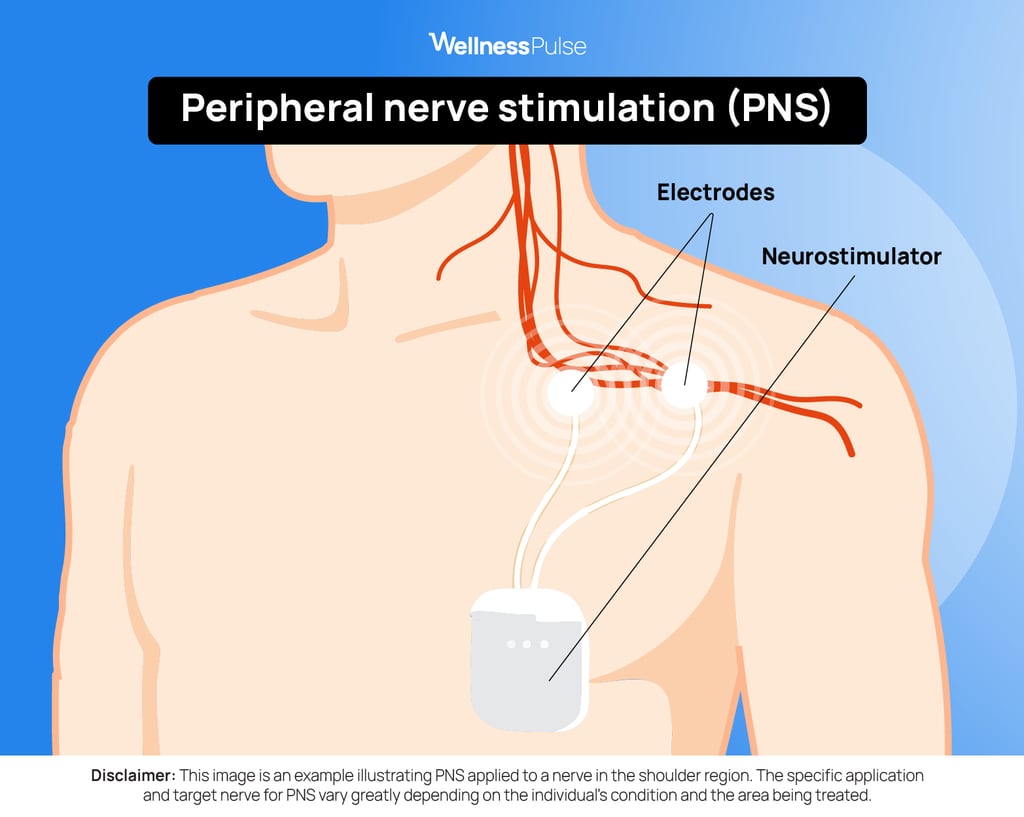
PNS is utilized to treat persistent pain confined to a localized region, like a shoulder, part of the skin, or an unrecovered nerve after trauma or surgery. It works by implanting a very thin wire just near the nerve in question.
How it works
Nerves are supposed to send useful messages, like when something’s too hot or when you’re injured. But sometimes, even after the tissue has healed, the nerve keeps sending pain signals that are no longer helpful. PNS steps in by giving the nerve a consistent, mild stimulation. Over time, this can help the brain interpret those signals differently, making the pain feel less intense or less constant.
Who it’s for
PNS is often considered when the pain is well-defined and hasn’t improved with medication, physical therapy, or injections. It’s most commonly used for:
- Pain after joint or soft tissue surgery
- Occipital neuralgia (pain at the back of the head)
- Localized back or leg pain that didn’t respond to surgery
- CRPS affecting a specific limb
- Nerve injury after trauma
What the process looks like
The first step is a trial. A temporary wire is placed near the nerve under imaging guidance, and an external device is used for a few days. If it helps, a permanent version can be implanted — usually through a small outpatient procedure.
The implant is discreet and adjustable. Individuals are given a small remote to manage the stimulation level, though many find one setting that works and leave it alone.
What sensations might you experience?
Most people do feel something when their neurostimulator is activated, although it is not intended to be painful. It may feel like a slight buzzing or a tingling that comes and goes. Sometimes, it follows a nerve pathway, like down the leg or through the arm. Sometimes, as with transcutaneous electrical nerve stimulation, it’s more subtle, a momentary shift in your voice or a flicker in your throat. And in some cases, like deep brain stimulation, there’s nothing you feel at all — just the effect over time.
It does take some adjusting to get the settings right, but that is all part of the process. The handheld controller lets you turn the stimulation up or down.
The goal isn’t to make you aware of the device every moment; it’s to set it to a level that helps without getting in the way.
Is neurostimulation safe?
No medical treatment is entirely without risk, and neurostimulation is no exception, but in the hands of the right team and for the right person, it’s generally safe and well-tolerated.
That said, implants do come with the kinds of issues you’d expect when you’re placing a device in the body. Some people experience soreness where the device or wires sit. In some cases, the lead — that thin wire doing the actual work — can shift slightly or need adjustment. Research shows that infections around the implant site are the most common side effects, though with proper care and follow-up, they’re usually caught early.
Certain systems, especially the ones that sit closer to the surface of the skin, like peripheral or subscalp devices, tend to have a slightly higher chance of irritation or movement; not usually dangerous, but worth keeping an eye on. Manufacturers are working on better designs to reduce this, and newer models are already seeing fewer of these problems.
There are people for whom neurostimulation is not advisable. If someone has a bleeding disorder, an active infection, or a specific type of heart device that doesn't coexist well with neurostimulators, it may be best to think about alternate options. That’s why the screening process is thorough — it’s about making sure the device helps more than it complicates.
In short: no, it’s not risk-free, but for many, the trade-off between manageable side effects and daily relief might be worth it.
Expert insight
When prescribing neurostimulation treatment for chronic pain, Costello looks at “threshold persistence, pain mapping clarity, and prior response patterns. If pain lasts beyond 180 days with consistent localization, and if three or more oral medications have failed without meaningful relief, then the probability of neural desensitization becomes clinically relevant.”
“At that point,” he adds, “neuromodulation may interrupt the loop. Factors like cognitive flexibility, sleep stability, and emotional regulation heavily influence whether the results will sustain past 12 months. Neurostimulation is not a cure, but when timed and framed well, it can widen the bandwidth for recovery.”
The bottom line
If you’ve been living with pain that doesn’t ease up or with a condition that keeps interrupting how you move, feel, or focus, it’s worth having a proper conversation about what’s next. Neurostimulation isn’t for everyone, but for some, it opens a door that felt long closed.
Sit down with a healthcare provider who knows your story — your history, your past treatments, what’s worked, and what hasn’t — and determine whether this option fits into the bigger picture of your care. Sometimes, knowing it’s even on the table changes the way forward. Sometimes, it’s the step that finally makes space for things to feel a little more manageable again.
It starts with a question. Ask it.
FAQ
Will I become dependent on my neurostimulator?
Not in the way people worry about with medications. Neurostimulators don’t create tolerance or withdrawal. You’re not ‘hooked,’ and if the day comes when you don’t want or need it, most systems can be turned off or removed.
Can I go through airport security with one?
Yes, but you’ll need to show your device card or medical ID. Security scanners can sometimes interfere slightly with the settings, but they don’t harm the device itself. Most people pass through with no issue at all, especially with newer systems.
What happens if the battery runs out?
Most implants use rechargeable batteries or ones that last several years. You’ll be told how to check levels and recharge when needed. If replacement is ever necessary, it’s usually a straightforward outpatient procedure, not starting over from scratch.
10 resources
- Surgery (Oxford). An overview of the nervous system.
- Neuroscience & Biobehavioral Reviews. A century of research on neuromodulation interventions: a scientometric analysis of trends and knowledge maps.
- Bioelectronic Medicine. Spinal cord stimulation in chronic pain: evidence and theory for mechanisms of action.
- Brain Spine. Real-world evidence on spinal cord neuromodulation and pain: long-term effectiveness analysis in a single-center cohort.
- Journal of Clinical Medicine. Deep brain stimulation for tremor: update on long-term outcomes, target considerations and future directions.
- Nature Medicine. Chronic adaptive deep brain stimulation versus conventional stimulation in Parkinson's disease: a blinded randomized feasibility trial.
- Epileptic Disorders. Outcome of vagus nerve stimulation for drug-resistant epilepsy: the first three years of a prospective Japanese registry.
- The American Journal of Psychiatry. A 5-year observational study of patients with treatment-resistant depression treated with vagus nerve stimulation or treatment as usual: comparison of response, remission, and suicidality.
- Epilepsy Research. Designing next-generation subscalp devices for seizure monitoring: a systematic review and meta-analysis of established extracranial hardware.
- StatPearls. Parkinson disease.





Your email will not be published. All fields are required.